Prosthetic Replacement
As the reconstruction of multiple fragment fractures may not be possible specifically in osteoporotic bone, cemented prosthetic replacement in complex C fractures during pre-operative planning must be considered. Reconstruction may not be preferable in case of little or no soft-tissue associations to the main head fragment in aged patients. In such conditions, results are better after primary head replacement as compared to secondary head replacement because after prosthetic replacement or with stable fixation only functional treatment can be allowed. Thus, a wide range of orthopaedic implants is available for the treatment of various fractures.
Surgical treatment of extra-articular unifocal A fractures
A1 fractures
In the case of unifocal fractures with greater tuberosity, treatment should be done by sling immobilization in the following situations:
-
In case of less than 40° angulation of the fragments.
-
In the case of younger patients if they are undisplaced or not more than 5 mm displaced.
-
In the case of elderly patients (60 and above), if they are not more than 10 mm displaced.
X-rays in internal and external humeral rotation are helpful in proper verification of displacement of tuberosity fragments.
A2 fractures
Sling immobilization should be used in case of surgical neck or sub-capital fractures without major displacement (less than 10 mm and angulation below 30º to 45º) but it depends on the patient’s age. After that passive motion, followed by active motion, can be prompted carefully. Functional treatment can be done after a few days if the fracture is impacted with an acceptable amount of varus or valgus malalignment considering the patient’s age.
A3 fractures
Re-displacement occurs in these unstable fractures whether they are impacted or can be reduced closed which results in stiffness, prolonged pain, and immobilization.
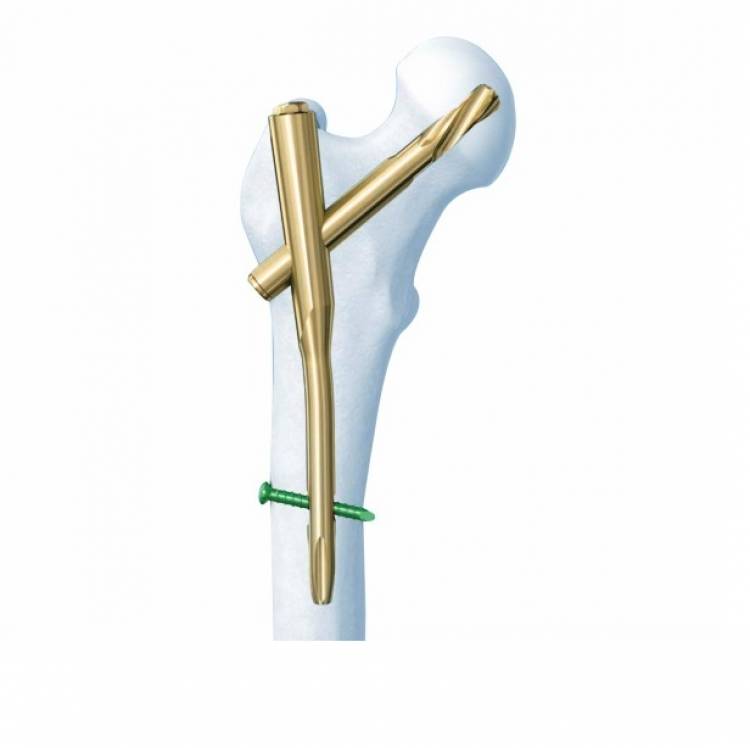
If they can be reduced, generally, percutaneous pinning under general anesthesia is performed for the maintenance of the reduction. As an alternative, in place of simple pinning, the use of 7.0 or 4.5 mm cannulated screws following the optimal placing of, generally, three 1.6 mm K-wires is recommended. These screws are inserted with power after the opening of the lateral cortex with a 4.5 mm drill bit but a 3.2 mm drill bit in the case of younger patients. Two from the lateral cortex and one from anteriorly are driven towards the head center.
To impact the fracture, one or two long cannulated cancellous bone screws are inserted and one or two K-wires can be inserted from the greater tuberosity into the medial shaft cortex. A passive motion under image intensification after the removal of the K-wire confirms the stability of fixation for post-operative functional treatment.
After the reduction, the other method of fixation is the use of intramedullary nails or pins, normally through retrograde insertion from about 3 cm proximal to the olecranon tip. Sufficient stability is provided by unreamed interlocking nails in A3.3 fractures with metaphyseal comminution. An external fixator is used in case of severe open comminuted, and contaminated fractures.
Usually, the interposition of the long biceps tendon, buttonholing through a split muscle or interposed fragments are the major reasons for the inability to reduce the fracture with the help of closed means. In such conditions, a deltopectoral approach is carried to correct the situation. Valgus impaction of up to 10º is acceptable and lag screws and/or plates can be applied for stable fixation. Usually, a 3-hole or 4-hole T-plate is inserted. Bone cement may be put into the drill holes if the anchorage of the screws is unreliable. Before closing the wound, the reduction, screw position, screw length, and stability must be checked using an image intensifier. This method is also useful for the stabilization of pathological fractures.
Longer T-plates bridging the medial comminution zone will be used in case of multi-fragmentary fractures at the surgical neck area or fractures extending further into the shaft. In such conditions removal of the anterior part of the deltoid insertion is acceptable. It needs to be sutured back.
The deltopectoral approach is used in case of open reduction. Tension-absorbing sutures or wires around the tuberosity fragments need to be anchored to screw heads or in plate holes. In multi-fragmentary fractures (B2.3) plates will be used routinely, However, in the case of type B fractures, the residual blood supply to the head must not be damaged.
If stable fixation is not possible to achieve, in these three-part fractures then hemiarthroplasty can be done for restoration.